Trust your body, outsmart the marketing:
comprehensive guide to choosing a therapist
Published 25 February 2026
22 minutes read
A practical guide to choosing a therapist when you are neurodivergent, questioning, burnt out, masked to the bone, or tired of explaining yourself
There is no cheat code for finding the best therapist.
Anyone promising certainty is selling you comfort, not care.
The good news is that you can get much better at choosing well. Therapy fit is not mystical. It shows up in your body, in the therapist’s behaviour, and in the tiny details of how the work is run.
For neurodivergent clients, especially autistic, ADHD, AuDHD and otherwise non-standard nervous systems, fit is not a luxury. It is part of safety. A therapist can be warm, experienced, highly trained and still be wrong for you if they misunderstand your communication, overload your senses, reward masking, or interpret neurodivergent processing as pathology.
This guide is here to help you do two things at once:
- trust your nervous system: your body’s early-warning system for safety, overload and mismatch
- outsmart the marketing: so you do not end up paying for a glossy therapeutic mismatch
This article uses therapy modality labels where helpful, but it treats them as descriptors, not destiny. CBT, EMDR, psychodynamic therapy, ACT, IFS, DBT, somatic work, person-centred therapy and coaching-style approaches can all be helpful or harmful depending on formulation, adaptation, pacing, power and fit.
The question is not only: Which therapy is evidence-based?
The better question is:
Evidence-based for whom, delivered by whom, with what assumptions, and adapted how?
Therapy is not a product. It is a relationship with a job.
Most purchases are simple. You buy an object. You own it. You move on.
Therapy is different. You are hiring a human to do skilled relational work with your mind, body, history, relationships and nervous system. You cannot separate the “service” from the person providing it.
That is why “nice” is not enough.
A therapist can be kind, friendly and credentialled, yet still leave you feeling smaller, more confused, more masked or more ashamed. For neurodivergent clients, mismatch often follows predictable patterns: differences in communication style, sensory load, predictability needs, power dynamics, processing speed, interoception, alexithymia, monotropism, rejection sensitivity, and the hidden cost of performing “good client” behaviour.
A clean definition:
Good-fit therapy helps you become more you, not more acceptable.
It does not train you into a more socially convenient version of distress.
Fit is not mystical. It is measurable.
Let’s make this satisfyingly unromantic.
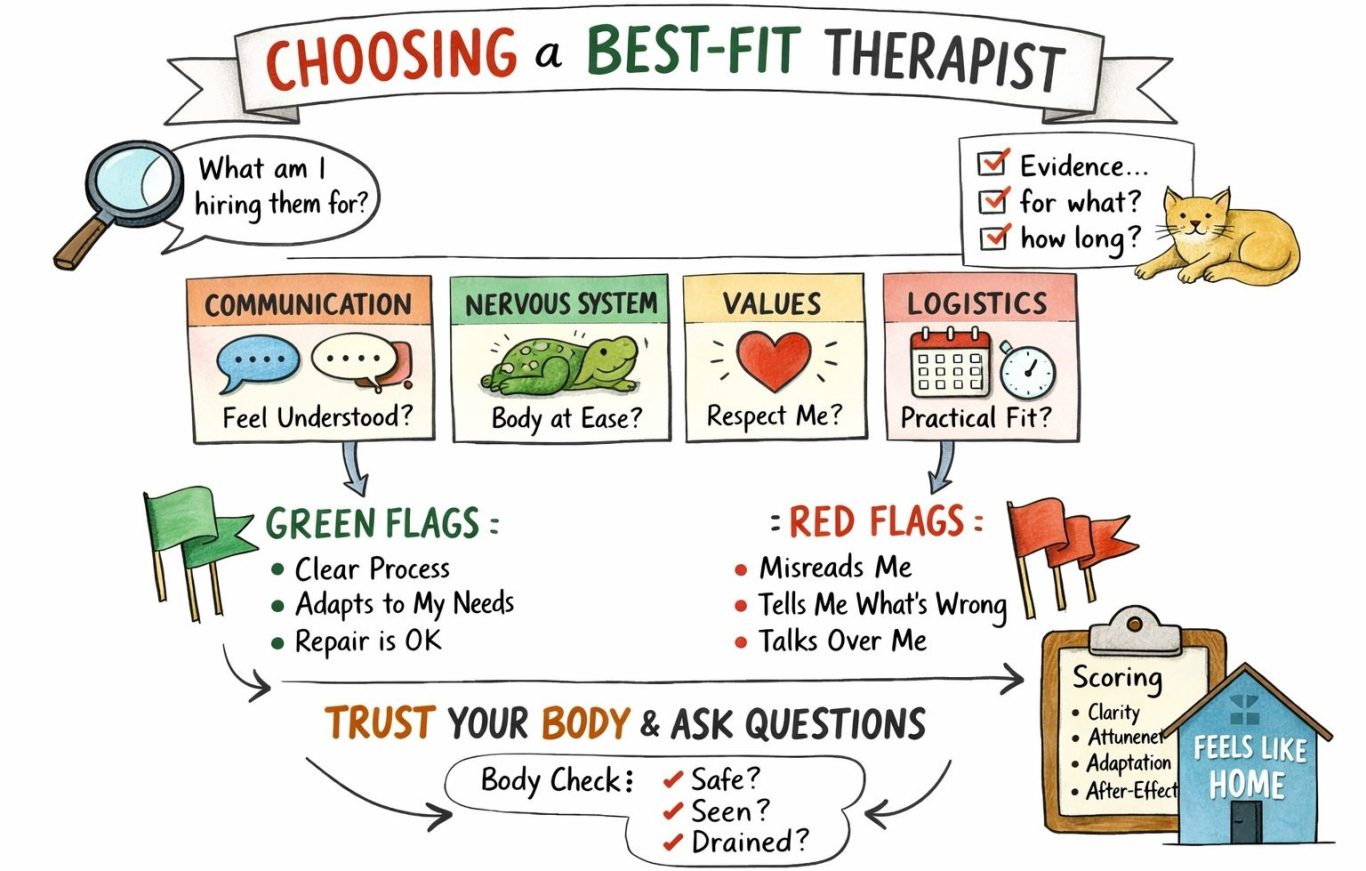
Fit = Communication + Nervous system + Values + Logistics
If one part is badly off, therapy can look good on paper and feel awful in practice.
1. Communication fit: do you feel understood without translating yourself into therapist-speak?
Neurodivergent communication can be direct, detailed, literal, pattern-based, tangential, slow-to-start, fast-to-connect, image-based, body-based, concept-heavy, non-linear, blunt, quiet, written, delayed, scripted or “too honest” for polite culture.
Some people need time before they can speak. Some need precise questions. Some need a written agenda. Some need summaries and meaning-checks. Some think in systems, not stories. Some need to info-dump before they can locate the emotional thread.
A good-fit therapist does not treat this as a problem.
They treat it as your interface.
Signs of communication fit:
- you do not leave feeling you must rehearse how to speak “correctly” next time
- they check understanding instead of guessing your meaning
- you can be precise without nuance being punished
- silence and processing time are respected
- you can correct them without them becoming defensive
- they ask questions that clarify rather than corner
- they understand that “too much detail” may be pattern recognition, not avoidance
If you frequently think, That is not what I meant, and they keep insisting their interpretation is the deeper truth, that is not depth.
It is a misunderstanding loop with a power imbalance.
2. Nervous-system fit: does your body settle in their presence?
Therapy is not just ideas. It is physiology.
Your nervous system is the first witness to safety.
For neurodivergent clients, nervous-system fit often hinges on sensory load and predictability:
- lighting, noise, temperature, smells, texture, visual clutter
- pace of speech
- abrupt topic changes
- vague or ambiguous questions
- pressure to make eye contact
- comfort with stimming, fidgeting, moving, looking away, using a blanket, sipping a drink, taking notes, typing, pausing, or asking for a break
You are not being “difficult” if you need a space that does not scramble you.
You are being practical about access.
A useful rule:
If the room makes you shrink, your brain has less room to think.
A therapist does not have to get every sensory detail perfect. But they do need to believe you, adapt where possible, and not treat your access needs as symbolic material to interpret before accommodating.
3. Values fit: are they aligned with your autonomy and identity?
Values mismatch can hide behind warmth.
For neurodivergent clients, values fit includes whether the therapist:
- treats neurodivergence as difference, not defect
- respects self-definition and lived experience
- understands that “functioning” is not the same as “well”
- does not reward masking as progress
- sees behaviour in context, not as a moral failure
- understands that distress may be sensory, relational, executive-function-related, trauma-related, systemic, medical, or environmental before it is “cognitive distortion”
- can distinguish safety from compliance
Watch for subtle cues.
Do they talk about “fixing”, “normalising”, “appropriate behaviour” and “social skills” as universal goals?
Or do they talk about quality of life, agency, energy, access, self-understanding and relational repair?
A therapist who wants you to look better at the cost of feeling worse is not necessarily helping you.
4. Logistics fit: does the admin support you or drain you?
This is the underestimated deal-breaker.
Booking, payment, reminders, cancellations, forms, waiting lists, location, technology, response times, and session timing are not separate from therapy. They are part of the service.
If the admin repeatedly destabilises you before you even start, therapy begins already taxed.
Neurodivergent energy is not infinite. Friction costs matter.
A therapist can be brilliant, but if their system repeatedly creates avoidable stress, confusion, shame or executive-function load, that is still relevant information.
Ask:
- Is the booking process clear?
- Are fees and cancellation policies explicit?
- Can I email rather than phone?
- Are reminders available?
- Do I know what happens in the first session?
- Is the location or online setup manageable?
- Do I know what to do if I am overloaded, late, shut down, or unable to speak?
Access is not a bonus feature. It is the doorway.
Why this matters: therapy can harm when autism is misunderstood
This is not just a matter of personal preference.
Emerging research on autistic adults’ therapy experiences repeatedly points to the same problem: therapy becomes unsafe when clinicians apply neurotypical assumptions to autistic nervous systems.
In a UK study in Counselling and Psychotherapy Research, Jones, Hamilton and Kargas explored neurodivergent clients’ counselling experiences and found recurring issues with confusing language, uncertainty, masking, sensory environments, and the need for clearer, more flexible, neurodivergence-informed counselling. The paper’s practice recommendations include collaborative work with neurodivergent clients, direct and flexible communication, neurodivergent-informed training, information about the counselling process in advance, and explicit questions about physical, environmental and communication accessibility needs. Jones, Hamilton & Kargas, 2025
A separate UK study in the same journal, by Di Marco, Wood and Troop, interviewed autistic adults who had accessed NHS psychological therapies. All participants reported a lack of psychological safety around autistic identity and named lack of therapist knowledge of neurodiversity as a barrier. The authors concluded that therapies were often experienced as harmful to autistic participants’ sense of identity, with some people feeling defective or as though the models used were not created for their brains. Di Marco, Wood & Troop, 2025
This matches autistic-led work from Hallett and Kerr, whose survey of autistic adults’ counselling experiences found repeated barriers around sensory access, communication, misunderstanding, outdated autism knowledge, and autistic struggles being dismissed or reinterpreted. Their recommendations are beautifully practical: believe autistic distress, adapt communication, understand meltdowns, shutdowns, burnout, alexithymia, processing time, executive functioning and the double empathy problem, and learn from autistic-led writing and training. Hallett & Kerr, 2020
This is the clinical risk:
If a therapist does not understand autism, the client may spend therapy explaining stimming, masking, sensory needs, shutdown, burnout, literal processing, executive dysfunction, monotropism or social exhaustion — instead of receiving therapy.
Worse, the client may be told they are “overthinking”, “resistant”, “avoidant”, “too sensitive”, “not trying”, “intellectualising”, “controlling” or “not engaging”, when what is actually happening is autistic processing, sensory protection, trauma-shaped caution, or a nervous system trying not to collapse.
That is not therapeutic depth.
That is clinical mislabelling.
Outsmart the marketing: when everyone says “evidence-based”
“Evidence-based” can mean something real.
It can also be used as a prestige badge.
The phrase sounds like safety, but evidence is never a single thing. It is evidence for a specific outcome, in a specific timeframe, with a specific group, delivered by particular practitioners, measured in a particular way.
So instead of being hypnotised by the label, translate it into grounded questions.
- Evidence for what?
Symptom reduction? Relationship improvement? Trauma recovery? Reduced avoidance? Less self-harm? Day-to-day functioning? Self-understanding? Quality of life? Autonomy? Lower masking? Increased access? Fewer shutdowns? Better sleep? More sustainable routines?
Those are not the same outcome.
A therapy that reduces visible distress by increasing masking may look successful from the outside and be destructive from the inside.
- Evidence over what timeframe?
Some changes are quick. Others are slow and layered.
Short-term outcome measures do not automatically tell you what happens after six months, after burnout, after returning to work, after a family conflict, after sensory load increases, or after the client stops performing “I am doing better” for the therapist.
- Evidence with whom?
Was the evidence gathered with autistic adults? Late-identified women? High-masking people? People with alexithymia? People with trauma histories? People with ADHD? People with learning disabilities? People from marginalised communities? People who communicate differently? People who shut down rather than outwardly express distress?
A method can be evidence-based and still poorly fitted to you without adaptation.
- Do they talk about relationship and process, or only outcomes and techniques?
If a therapist profile reads like a menu of problems they can “treat”, be cautious.
If it reads like a thoughtful description of how they work with a person, adapt, check understanding, repair ruptures and respond to difference, that is often a better sign.
The punchline:
Good therapy is not just evidence-driven. It is person-responsive.
The central risk: mistaking neurodivergence for distortion
A familiar pattern shows up across clinical experience, research and lived-experience accounts.
Therapy becomes harmful not simply because of what it is called, but because clinicians misread neurodivergent realities as pathology, resistance, avoidance, faulty thinking, trauma reenactment, personality difficulty or lack of effort.
Examples:
- sensory pain is interpreted as avoidance
- executive dysfunction is mistaken for fear, depression or noncompliance
- autistic burnout is treated as ordinary low mood
- shutdown is read as withholding
- direct communication is read as hostility
- delayed processing is read as disengagement
- stimming is treated as a symptom to reduce rather than regulation to respect
- social caution is labelled irrational anxiety when it may be a proportionate response to repeated misunderstanding, rejection or overwhelm
- the need for predictability is interpreted as “control”
- a person’s need to understand the mechanism is interpreted as intellectualising
In other words, the problem is often not “your beliefs”.
The problem may be your body, your environment, your energy budget, your communication context, your access needs, or your history of being hurt in predictable ways.
A concrete example: the dishes problem
A person is told for years that difficulty doing the dishes must reflect avoidance, laziness, trauma, fear of responsibility, depression or “not caring”.
But in reality, the task involves severe sensory distress: sound sensitivity, aversive textures, heat, splashing, bright lighting, unpredictable water temperature, smell, visual mess, and the “ick” factor of food residue.
If therapy targets “avoidance” without understanding the sensory load, it increases shame and does not solve the problem.
If the sensory barriers are reduced — gloves, softer lighting, soaking, a dishwasher, noise reduction, different timing, breaking the task into smaller steps, body-doubling, visual prompts, or sharing the task differently — the person may suddenly become “more capable”.
They were not morally improved.
The environment stopped attacking them.
The lesson is simple:
If therapy targets the wrong problem, it increases shame instead of reducing suffering.
Therapy modalities and neurodivergent clients: what helps, what harms, and why fit matters more than brand
Mental health care for neurodivergent people is often discussed as if the key question is which modality is “best” or “worst”.
A more useful question is:
What happens when therapy is applied through neuronormative assumptions, and what changes when therapy is adapted in a neuroaffirming way?
- CBT: structured, practical, and potentially invalidating
- CBT can help when structure provides:
- clarity about what is happening and why
- explicit goals
- predictable pacing
- practical tools without blame
- shared experiments rather than compliance tests
- attention to environment, body and access needs
CBT can harm when structure becomes:
- pressure to monitor and correct yourself constantly
- a subtle message that your perceptions are wrong
- homework that becomes proof you are “not trying”
- a demand to dispute realistic social or sensory threat
- a focus on thoughts while ignoring body, context and disability
For clients who already live under a masking tax, therapy should not become another self-surveillance project.
A useful question for any CBT-informed therapist:
How do you distinguish cognitive distortion from accurate pattern recognition, sensory threat or repeated relational injury?
If they cannot answer that, be cautious.
DBT: skills can help, assimilation can harm
DBT can be profoundly stabilising, especially for emotion regulation, distress tolerance, crisis survival and relationship skills.
Many neurodivergent people live with chronic invalidation, trauma, social stress and nervous-system dysregulation. Practical skills can be lifesaving.
But skills can become harmful when they are used to target neurodivergent traits rather than distress.
If “interpersonal effectiveness” becomes code for performing neuronormative behaviour, if “emotional regulation” ignores sensory overload, shutdown, meltdown and burnout, or if success is measured by looking less neurodivergent for other people’s comfort, then therapy becomes assimilation training.
A therapy that improves short-term conformity at the cost of long-term self-alienation is not necessarily a success.
Exposure therapies: danger when the target is misidentified
Exposure-based approaches can be effective when they target disproportionate fear and avoidance.
But there is a crucial caveat:
Exposure is dangerous when the thing being exposed to is genuinely painful, overwhelming or unsafe.
If a therapist treats sensory aversion, autistic burnout or social threat built from lived experience as irrational fear, repeated exposure may not build tolerance.
It may teach the client to override their body until the body refuses.
Careful formulation matters:
- Is this disproportionate fear or proportionate distress?
- Is this avoidance or a sensory boundary?
- Is this a phobia, or accumulated relational injury?
- Is this anxiety, or accurate prediction based on past harm?
- Is the nervous system learning safety, or learning helplessness?
Without those distinctions, exposure can become a sophisticated way of teaching clients to mistrust their bodies.
Psychodynamic and insight-oriented therapies: depth with projection risk
Psychodynamic, relational and other insight-oriented work can be deeply healing when it emphasises individuality, emotional validity, mutual reflection, repair, meaning-making and the complexity of relational life.
The risk comes when a therapist relies heavily on symbolism, inference or hidden motives, then treats their interpretation as more real than the client’s lived experience.
Neurodivergent communication may be mislabelled as defensiveness, detachment, intellectualisation, rigidity or unresolved conflict when it may simply be a different style.
A good therapist can wonder without colonising.
The guiding principle:
Interpretation should never outrank the client’s self-knowledge.
Somatic therapies, EMDR, ACT, IFS, narrative and creative approaches: often valued, not automatically safe
Many neurodivergent clients value approaches that make room for embodiment, nervous-system regulation, values, parts, imagery, memory processing, creative expression and non-verbal routes into meaning.
These approaches can be powerful precisely because they do not rely exclusively on verbal analysis.
But “powerful” is not the same as “universally safe”.
Anything that moves the nervous system can overwhelm it if sensory processing, dissociation risk, alexithymia, communication differences and pacing are not respected.
Good questions to ask:
- How do you pace trauma or body-based work with autistic or ADHD clients?
- What happens if I go blank, freeze, shut down or cannot describe what I feel?
- Can we work with images, words, body signals, notes, movement, silence or metaphor depending on what is accessible that day?
- Do you treat stimming and movement as regulation rather than disruption?
The method matters.
The adaptation matters more.
Practitioner fit may matter more than modality fit
Across the best clinical thinking, the conclusion is consistent:
- a rigid, poorly informed therapist can misuse almost any approach
- a flexible, collaborative, neuroaffirming therapist can often adapt even structured work in helpful ways
So instead of shopping for a label alone, shop for a clinician who works with your neurotype rather than against it.
Ask yourself:
- Do they trust my account of my inner world?
- Do they distinguish sensory pain from fear?
- Do they distinguish burnout from depression?
- Do they understand shutdown, meltdown and masking?
- Do they treat stimming as regulation, not misbehaviour?
- Do they treat social caution as potentially realistic, not automatically distorted?
- Do they aim for reduced suffering and increased agency, or for normative performance?
- Can they handle direct feedback without becoming defensive?
These questions cut across every brand.
A spicy reality check about money
Your nervous system does not live on fairy tales.
There is a persistent cultural myth of the saintly therapist in a shabby room who can heal you for the price of a sandwich. It is a nice story. It is also a risky way to choose care.
A therapist does not need to be wealthy to be good, and high fees do not guarantee competence. But chronic undercharging and constant financial strain can be a red flag.
Good therapy requires time, supervision or consultation, ongoing training, administrative clarity, enough personal bandwidth to think carefully, and recovery space between emotionally demanding sessions.
If a clinician is permanently scrambling to survive, cutting corners on learning and support, or booking back-to-back sessions with no thinking room, your work can quietly become collateral damage.
A grounded way to use money as information:
- be wary of prices that look like a bargain because the therapist is desperate, not because they have chosen an accessible model
- ask about supervision, consultation and continuing professional development
- notice how the therapist talks about boundaries
- notice whether fees and policies are clear rather than vague or apologetic
Think of fees as one data point about resources and sustainability — not as moral judgement, and not as proof of brilliance.
Your goal is simple:
Someone resourced enough to do careful work, and transparent enough to talk about it.
The consultation: how to choose well in real life
A first call is not an audition.
It is a compatibility check.
You are not trying to impress them. You are observing how they think.
Questions about process
- “What tends to happen in your first few sessions?”
- “How do we keep track of whether this is helping?”
- “What do you do when therapy is not working for someone?”
- “How do you handle misunderstandings in the room?”
Questions about adaptation
- “What adjustments do you commonly make for autistic, ADHD or otherwise neurodivergent clients?”
- “If I need more directness or structure, can you work that way?”
- “Can I use notes, email, movement, stimming, silence or written processing?”
- “Can we agree what to do if I shut down or cannot speak?”
Questions about safety and pacing
- “How do you pace work so it does not overwhelm me?”
- “If I become overloaded, how would we handle that?”
- “How do you distinguish trauma avoidance from sensory boundaries?”
- “How do you work with autistic burnout?”
Questions about values
- “What does neurodivergence mean to you in therapy?”
- “What is your view on masking and unmasking?”
- “How do you think about social skills work?”
- “How do you make sure therapy does not become normalisation?”
What you are listening for
- specificity, not slogans
- humility, not certainty
- curiosity, not judgement
- collaboration, not control
- adaptation, not “we treat everyone the same”
- repair, not defensiveness
You do not need the therapist to know everything.
You need them to know enough, learn well, believe you, and not make you pay session after session to educate them on the basics.
Trust your nervous system without letting anxiety run the whole show
Nervous-system signals are real.
They can also be noisy.
Past experiences can make safety feel unfamiliar, and unfamiliar can feel unsafe. Trauma, rejection sensitivity, burnout, medical trauma, previous therapy harm and long-term masking can all make the body brace early.
So do not rely on one feeling.
Rely on patterns.
After any consultation or early session, do a quick body-and-brain debrief:
- Did my body soften at any point, even briefly?
- Did I feel seen, or analysed?
- Did I understand what we were doing?
- Did they adapt to me in real time?
- Could I correct them?
- Did I feel more choice, or less?
- How did I feel later that day and the next day?
- Was I usefully tired, or wrecked?
If your body repeatedly says “brace”, and the therapist repeatedly says “this is just resistance”, pay attention to the brace.
Your body may be picking up a mismatch before your polite brain has permission to name it.
A simple scoring system because feelings are real and numbers help
After each early session, rate 0–2 on each area.
Clarity
Did I understand the purpose and direction?
0 = no
1 = partly
2 = yes
Attunement
Did they seem to understand me without forcing translation?
0 = no
1 = partly
2 = yes
Adaptation
Did they adjust to my needs and signals?
0 = no
1 = partly
2 = yes
Agency
Did I feel more choice, not less?
0 = no
1 = partly
2 = yes
After-effect
Was I usefully tired rather than destabilised, shamed or wrecked?
0 = no
1 = partly
2 = yes
Score out of 10.
Repeat for three sessions if possible.
This is not cold.
It is kind.
It protects you from staying in something that looks respectable and feels harmful.
If you are already in therapy and it feels off: try a repair before you run, unless you need to leave
Leaving is allowed.
Trying a repair is also allowed.
The key is agency.
A simple three-step approach:
1. Name it plainly
- “I often leave feeling confused.”
- “I need more structure.”
- “I feel like I have to perform in here.”
- “I do not think you understood what I meant.”
- “When you called that avoidance, I felt misread. I think it is sensory overload.”
2. Request an adjustment
- “Could we start with a brief plan?”
- “Could you summarise what you are hearing and check it with me?”
- “Could we slow the pace and focus on one thread?”
- “Could we use written notes or a shared agenda?”
- “Could we make a plan for what happens if I shut down?”
3. Watch what happens next
Curiosity and adaptation are green flags.
Defensiveness and dismissal are red flags.
A therapist does not need to be perfect. They do need to repair.
If they cannot tolerate being corrected, they are asking you to fund their authority problem.
Red flags and green flags
Red flags
Be cautious if a therapist:
- describes your access needs as avoidance before understanding them
- treats eye contact, tone or facial expression as proof of your inner state
- says they are “neurodiversity-affirming” but cannot describe actual adaptations
- repeatedly tells you that you are overthinking when you are trying to process accurately
- interprets stimming, silence or looking away as disrespect or resistance
- pathologises directness without checking meaning
- treats autism as either tragedy or superpower
- seems threatened when you know research, terminology or your own patterns
- wants you to “function better” without asking what functioning is costing you
- makes you feel you must become easier for others rather than safer in yourself
Green flags
Look for a therapist who:
- asks what helps you communicate
- gives clear expectations
- welcomes correction
- checks understanding
- understands sensory load and executive function
- can discuss masking, burnout, meltdown and shutdown without panic or judgement
- treats stimming and movement as regulation
- can hold trauma and neurodivergence together without collapsing one into the other
- understands that disability access is not avoidance
- is willing to adapt the room, pace, structure and modality
- speaks with humility about what they know and what they are still learning
A strong green flag:
You feel less pressure to translate yourself into a more acceptable format.
The final test: therapy should reduce your masking debt, not increase it
Neurodivergent people often survive by paying a daily masking tax.
Therapy should not add interest to that debt.
Good therapy does not begin with:
How do we make you less like this?
It begins with:
What is actually happening — in your body, your mind, your environment, your history and your relationships?
That shift from correction to understanding matters more than the label.
- Be choosy.
- Be practical.
Trust your body and interrogate the marketing. Both are forms of intelligence.
When you find the right person, therapy stops feeling like you are trying to become someone else.
It starts feeling like you are finally allowed to come home.
The information in this article is provided for general psychoeducational purposes only. It is not therapy, clinical advice, diagnosis, or a substitute for working with a qualified professional, and it should not be relied on as such. Any examples are illustrative and may not apply to your individual circumstances. If you are considering making changes to your health, wellbeing, relationships, work, or care, seek appropriate professional support tailored to you.
If you are in immediate danger or feel unable to keep yourself safe, contact emergency services or your local crisis support line straight away.
The information in this article is provided for general psychoeducational purposes only. It is not therapy, clinical advice, diagnosis, or a substitute for working with a qualified professional, and it should not be relied on as such. Any examples are illustrative and may not apply to your individual circumstances. If you are considering making changes to your health, wellbeing, relationships, work, or care, seek appropriate professional support tailored to you.
To the fullest extent permitted by law, we accept no responsibility or liability for any loss, harm, or outcome arising from reliance on the contents of this article. If you are in immediate danger or feel unable to keep yourself safe, contact emergency services or your local crisis support line straight away.
© Olena Baeva 2009-2026